
Is Length of Stay Still a Valid Measure in a Value-Based World?
// By Althea Fung //
 At the 2018 SHSMD Connections conference in Seattle, SHSMD convened a series of presentations on value as part of its “Value Initiative.” What does value mean for health care organizations? How can they achieve it?
At the 2018 SHSMD Connections conference in Seattle, SHSMD convened a series of presentations on value as part of its “Value Initiative.” What does value mean for health care organizations? How can they achieve it?
One of the presenters, Jessica Farrar, director of strategic planning and decision support at Anne Arundel Medical Center in Maryland, spoke about traditional metrics that don’t tell the whole story in a value scenario. Length of stay (LOS) has long been a mainstay in quality and efficiency measures, but does it leave out crucial information? What could you use instead?
In today’s value-based care environment, hospitals are under increased pressure to maintain quality while also lowering costs. Length of stay (LOS) is the duration of an inpatient episode of care, calculated from day of admission to day of discharge, and based on the number of nights spent in hospital. By tracking LOS, hospitals seek to improve processes and prevent errors, which ultimately lowers costs.
But for Anne Arundel Medical Center, a 350-bed hospital in Annapolis, Maryland, the LOS metric didn’t sufficiently capture the time a patient spent within the hospital walls.

Jessica Farrar, director of strategic planning and decision support, Anne Arundel Medical Center
“We found that [length of stay] is really clunky, in that it doesn’t allow us to look at detailed elements of a patient stay — places where there might be inefficiencies,” says Jessica Farrar, director of strategic planning and decision support at Anne Arundel Medical Center. Her team found that the wide view LOS takes misses fine details like performance differences between units and issues with discharge planning. It also misses a portion of the patient population that doesn’t fall under traditional metrics.
“[Length of stay] only counts inpatient, and hospitals now have patients in non-inpatient status who are in a room. We have patients who are observation status or patients who are technically outpatients that are postsurgical who recover in a room on a floor,” Farrar explains. “So we came up with a metric to really follow the patient — their physical presence as they moved through the hospital environment regardless of their status.”
Identifying Location and Care Gaps in Real Time
The program, called “Average Unit Stay,” follows a patient through his or her stay, taking note of the time the patient stays in each unit — not just the time spent from admission to discharge. Implemented in the summer of 2018, this program allows hospital staff to see location and care gaps in real time.
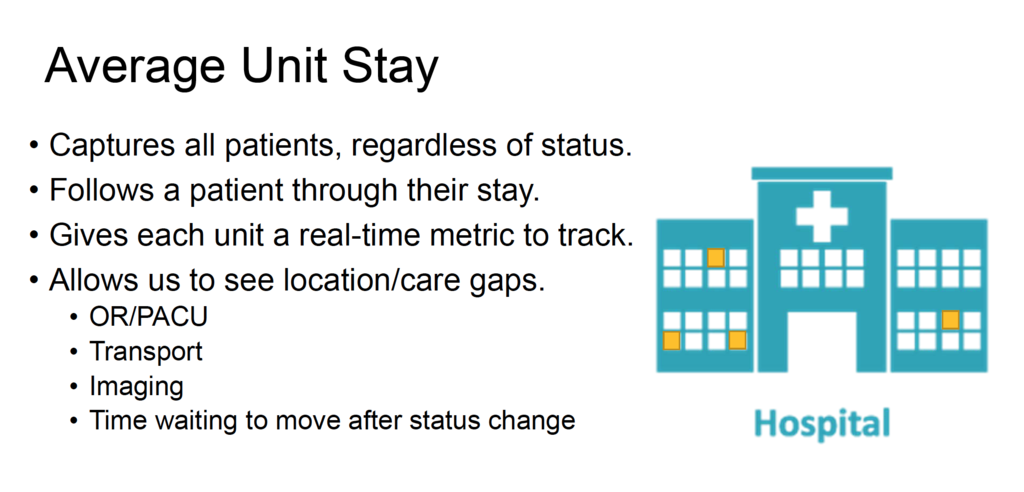
New metric accounts for all time spent in hospital
“This allows nurses in one unit to evaluate care provided in that unit and try to figure out if the amount of time a patient is spending in that unit is going up or down. It helps to identify inefficiencies — if there are inefficiencies. It allows for a much more detailed evaluation of the patient’s time spent in the hospital,” she says.
Educating Frontline Staff
To implement the program hospital-wide, departments throughout the hospital had to come together to effectively communicate the purpose and how the data gathered would be evaluated. The performance improvement department monitors units as the data is input into a platform that the IT department specifically created for this initiative. Also, department heads were tasked with educating frontline staff on what the metric means for their day-to-day work.
“We want to use this metric to evaluate performance to reduce length of stay. Ultimately, we want to be able to use this as a precise tool to help us with our staffing models and make sure we have the right staff on the right floors,” she says.
The Average Unit Stay metric is one of many initiatives that Anne Arundel Medical Center has implemented over the years aimed at improving quality and reducing costs.
New Insights Discovered
Since the Average Unit Stay program is just a few months old, Farrar says it’s difficult to calculate fiscal savings, though she says Anne Arundel Medical Center has already identified areas for improvement that could support hospital goals and global budget revenue or GBR goals in the long term. (For more on GBR, see box below.)
“Because we can see how a patient flows through the hospital, there were places where there are inefficiencies in discharge processes. We were able to identify units that were doing a good job managing that time and those that are slower to discharge. Once we can identify problems, we can come up with data solutions,” Farrar says.
Maryland Testing Ground for New CMS Payment System
Since the 1980s, Maryland has served as a testing ground for Centers for Medicare & Medicaid Services (CMS) cost-savings initiatives. The state, which has a Medicare waiver that allows it to adopt new policies, operates the only all-payer hospital rate regulation system in the country. Maryland is exempt from the Inpatient Prospective Payment System (IPPS) and the Outpatient Prospective Payment System (OPPS), and is allowed to set rates for those services.
In 2014, Maryland and CMS negotiated a new payment system for hospitals called the global budget revenue (GBR). The GBR changes the payment system from a fee-for-service system to a prepaid global budget set by the state’s HSCRC (Health Services Cost Review Commission). The GBR aims to:
- Decrease 30-day hospital readmission rates
- Decrease hospital-acquired conditions by 30 percent over five years
- Limit per capita growth to less than 3.58 percent
- Keep growth of Medicare spending to less than 0.5 percent below the national average
- Save Medicare $330 million over five years
This article is based on a presentation, “Strategically Addressing the Value and Affordability of Health Care,” at the SHSMD Connections 2018 conference.
Althea A. Fung is a digital content strategist and healthcare journalist. Reach her at fungus@altheafung.com.