
Rowing Together: A Collaborative Approach to Promoting Behavior Change
// By Susan Dubuque //
 As health care marketers, we are keenly aware of the rampant changes taking place in our industry — unforeseen mergers and consolidations, aggressive competitors entering the marketplace, pressures to demonstrate measurable ROI, and reorientation from delivering acute or episodic care to managing the health of a population with the goals of improving health and reducing costs.
As health care marketers, we are keenly aware of the rampant changes taking place in our industry — unforeseen mergers and consolidations, aggressive competitors entering the marketplace, pressures to demonstrate measurable ROI, and reorientation from delivering acute or episodic care to managing the health of a population with the goals of improving health and reducing costs.
Perhaps it is time that we create some of that change — time that we become the disruptors.
Let’s shake things up a little by changing the role of marketing in a population health world. By learning, adapting, and applying proven theories and models of behavior change, we can meaningfully participate, and even take the lead, in our organizations’ prevention and health enhancement efforts.
Historically, these activities have been the domain of clinical personnel with input from operations, quality assurance, utilization review, decision support, finance, and other team members who are concerned with outcomes and cost containment. Marketing and communications professionals have been conspicuously absent until the very end, when someone realizes, “Hey, we need to promote this program. Someone call marketing.”
But consider the value that marketing and public relations can offer in the initial design and early rollout of a population health initiative. In fact, let’s take it one step further. There are even more benefits to be gleaned when everyone is rowing the boat together — when we deploy a collaborative model for behavior change.
 Here, we’ll see how collaborative models can be structured for diabetes intervention, colon cancer prevention, and cardiac screening, and how UNC Health Care is teaming up with clinical partners to drive behavior change.
Here, we’ll see how collaborative models can be structured for diabetes intervention, colon cancer prevention, and cardiac screening, and how UNC Health Care is teaming up with clinical partners to drive behavior change.Let’s begin by looking at the contributions that marketing/communications and clinical team members can each bring to the party. For the sake of discussion, we’ll focus on nursing, but the same principles apply to any clinical discipline.
| Marketing/Communications | Nursing/Clinical Personnel |
|---|---|
|
|
Grounded in Theory
Designing a prevention or health improvement program may involve a significant investment of time and resources. Therefore, you want to increase your chances for success. And that’s possible if you build your program on a solid foundation of theory.
Behavioral change theories and models — borrowed largely from public health — can give you a richer understanding of how to motivate patients, your own employees, and the community as a whole to make changes for the better when it comes to health.
Three Approaches to Behavior Change
Here are three behavior change theories and models that lend themselves to a collaborative approach when applied in the health care setting.
1. Levels of Prevention
Prevention as a concept in population health means more than you may think.
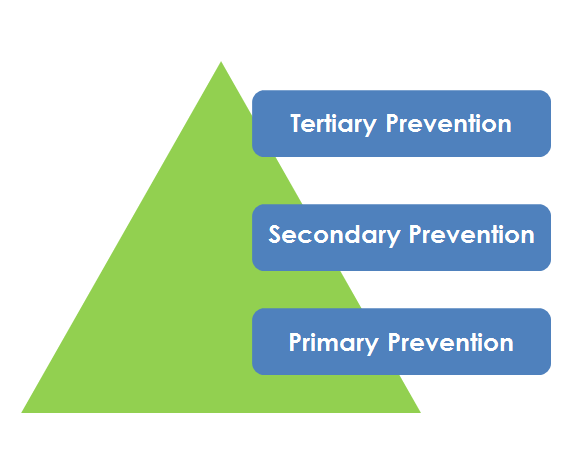
- Primary prevention refers to preventing a health problem or disease before it begins, such as immunizations, health education, and health policy.
- Secondary prevention involves at-risk populations and is designed to prevent the progression or recurrence of a disease or disability.
- Tertiary prevention refers to the management of chronic medical conditions.
Here is an example of a collaborative approach to developing a diabetes intervention program based on levels of prevention.
| Level of Prevention | Marketing/Communications | Nursing/Clinical Personnel |
|---|---|---|
| Primary | Produce promotional campaign to build awareness of risk factors and prevalence of diabetes | Conduct community health education programs and screenings for diabetes |
| Secondary | Launch a CRM campaign to recruit participants for a yearlong “Diabetes Prevention Lifestyle Change Program” | Conduct the prediabetes education program; counsel patients; monitor patient progress in reducing risk factors for diabetes |
| Tertiary | Design patient education materials; create a branded app (or other communications tool) for diabetic patients to track health habits and receive ongoing support from the clinical team | Provide ongoing disease management for patients diagnosed with diabetes; provide patient counseling; offer referrals to additional support services, e.g., exercise programs, support groups |
2. Social Ecological Model
The social ecological model is a means of articulating the social determinants of health and various levels of influence.
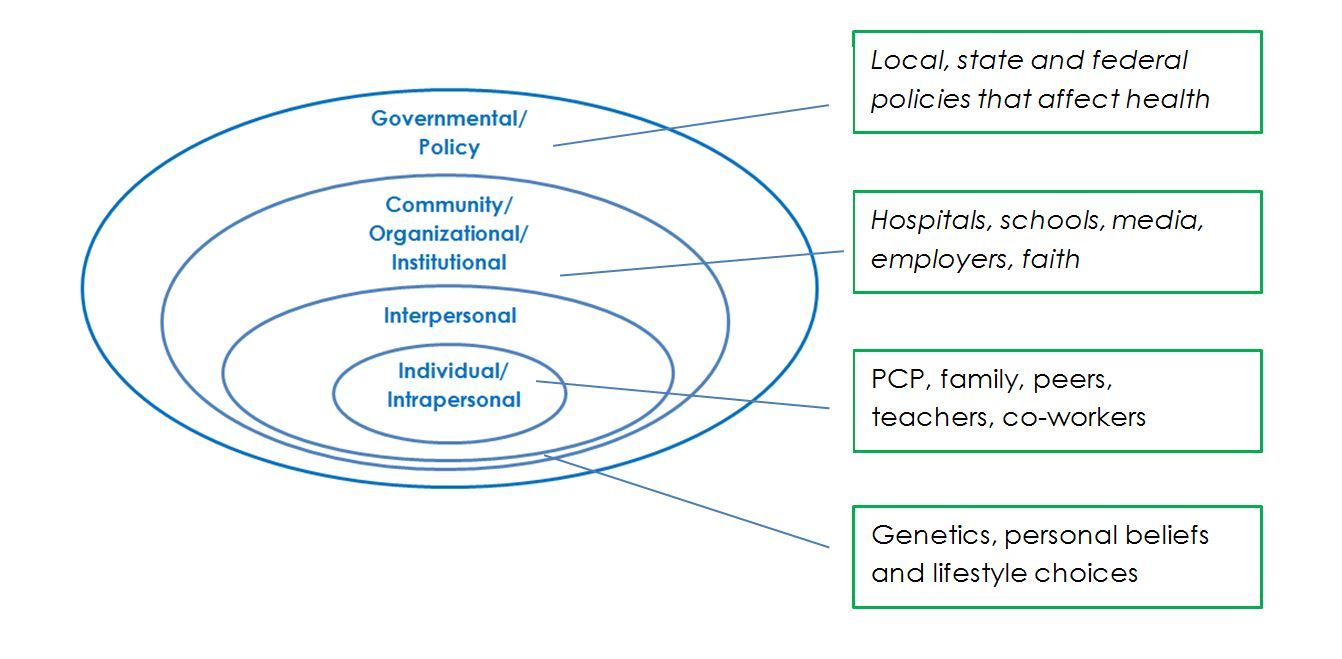
Below you will see how the marketing team and clinical services can work together to develop a colon cancer prevention program based on the social ecological model.
| Level of Influence | Marketing/Communications | Nursing/Clinical Personnel |
|---|---|---|
| Individual/Intrapersonal | Conduct focus groups with adults age 50+ to understand their level of awareness of colon cancer risks and prevention factors and identify barriers to having a colonoscopy | Provide clinical information; improve access to screening, such as through evening and Saturday hours, simplified scheduling |
| Interpersonal | Produce information kits, including posters and patient brochures, for physicians and their office staffs | PCPs discuss the importance of colonoscopy with their patients age 50+ (or younger if risk factors for colon cancer are present) |
| Community/Organizational | Develop a campaign in collaboration with health department, faith communities, and employers to educate the public about colon cancer risks factors and the importance of colonoscopy | Offer community education programs at churches, places of employment, and community centers to promote awareness of colon cancer risk factors and the importance of colonoscopy |
| Government/Policy | Communicate policy decisions to the public (e.g., insurance mandates for health screenings) | Clinical leadership advocates for policies to support greater access to health screenings and funding for the uninsured |
3. Transtheoretical Model: Stages of Change
Adopting a new health behavior rarely happens overnight or in one fell swoop. The Transtheoretical Model, called Stages of Change (SOC), is designed to help at-risk populations move through well-defined steps with the goals of reducing the health risk and converting the new behavior into a well-established habit.
This is accomplished by matching the stage — or state of readiness — with the appropriate message, media, and program for behavior change. SOC is at the core of customer relationship management (CRM) programs.
The Stages of Change model offers ample opportunity for the marketing and communications team and nursing and other clinical providers to contribute to a behavior change initiative.
Here are the six Stages of Change:

Depicted below is an example of SOC applied to a cardiac screening program.
| Move from Stage to Stage | Marketing/Communications | Nursing/Clinical Personnel |
|---|---|---|
| Precontemplation to Contemplation | Produce a campaign to build awareness of risk factors of heart disease and benefits of healthy lifestyle changes | Conduct learning needs assessment or provide generic information and content |
| Contemplation to Preparation | Offer a soft call to action such as attend a class or download a guide to healthy living | Deliver health education programs on Heart Healthy Living to help resolve ambivalence |
| Preparation to Action | Offer a hard call to action, such as: register for a cardiac screening | Conduct cardiac screenings; counsel patients identified with heart disease and refer them for follow-up care |
| Action to Maintenance | Promote programs to provide patients with support for positive behavior changes, such as support groups, and exercise programs | Offer ongoing support for patients who have made lifestyle changes; provide disease management for those who have been diagnosed with heart disease |
| Maintenance to Termination | Develop means of maintaining contact with patients, such as newsletters, email blasts; solicit testimonials, recommendations and referrals from patients who have successfully completed programs | Continue providing ongoing clinical care as needed; refer patients for other services (cross-selling) |
Collaborating to Create Sustained Behavior Change at UNC

Lisa Schiller, chief communications and marketing officer for UNC Health Care
Lisa Schiller, chief communications and marketing officer for UNC Health Care, has seized the opportunity to dovetail her department’s efforts with those of her clinical colleagues. “Our statewide marketing, communications, and patient experience teams meet biannually for health system updates and professional development,” she says. “The topic for our summer meeting was centered on population health and behavior change. For this particular subject, we expanded the invitation list to include team members from other disciplines, including nursing, performance improvement, and care redesign.”
From the clinical perspective, Julia Aucoin, DNS, RN-BC, CNE, director of practice, quality, and research for UNC Rex Healthcare, sees the respective — yet synergistic — roles of marketing and nursing in the following way: “Theoretically, nursing is patient-centric, while marketing is population-centric. In order to develop a comprehensive population health program, we have to consider behavioral change at both levels.”

Julia Aucoin, DNS, RN-BC, CNE, director of practice, quality, and research for UNC Rex Healthcare
Traditionally, nurses have focused on individual patient education to address core concepts needed by most patients with that medical condition,” Aucoin says. “Yet, this approach has not been successful in reducing readmissions. Behavior change takes time and requires reinforcement and rewards in order to be sustained. By shifting from patient education — checking the boxes — to behavior health management, we are no longer telling patients what to do. Rather we’re helping them see what they need to do to change their own situations. Nursing can then learn from our marketing colleagues how to extend this behavioral change approach from one-on-one to the population as a whole.”
“It is clear that in the future, and even today, collaboration among these groups is imperative for understanding consumer and patient motivations and behaviors,” Schiller adds. “Working together to influence positive health outcomes and wellness is truly the only way to create sustained behavior change.”
Susan Dubuque literally wrote the book on population health for marketers. Gearing Up for Population Health: Marketing for Change was published by SHSMD of the American Hospital Association in 2018. She is a principal and co-founder of twotango, a marketing and advertising firm based in Richmond, Virginia, and an adjunct professor at Virginia Commonwealth University in the Department of Healthcare Administration. Previously, she was the director of marketing for Mary Immaculate Hospital in Newport News, Virginia. Susan serves on the Editorial Advisory Board for Strategic Health Care Marketing.